UK Clinical Trials Reform 2026: ICH E6(R3) Now Legally Binding from 28 April
The Legal Position
The Medicines for Human Use (Clinical Trials) (Amendment) Regulations 2025 come into force, amending the Medicines for Human Use (Clinical Trials) Regulations 2004 (S.I. 2004/1031). For all CTIMPs conducted in the UK, compliance with the ICH E6(R3) Good Clinical Practice principles is now a statutory requirement under Schedule 1, Part 2 of those Regulations.
Schedule 1, Part 2 also retains three UK-specific requirements. Trials must comply with the principles of the Declaration of Helsinki, except where doing so would contravene the Regulations. Insurance or indemnity must cover liabilities arising for the investigator and sponsor. The investigator and sponsor must have regard to relevant guidance, including the E6(R3) and its annexes, where applicable.
MHRA is expected to assess wheather sponsors have evaluted the E6(R3) principles and can justify their approach at inspection. Annexe 1, documented the quality-system impact of that assessment, and be prepared to defend it at inspection.
The Quality Standard
E6(R3), read with ICH E8(R1), emphasises documented, trial-specific reasoning rather than reliance on standardised procedural volume. Three constructs now define the UK quality standard:
- Critical to Quality (CtQ) factors: the trial-specific elements where error or omission could materially impact rights, participant safety, rights, well-being, or the reliability, integrity and interpretability of results. Identified prospectively, and carried into the protocol, risk assessment, quality plan, and data management plan.
- Quality by Design: quality embedded at protocol design stage, before first enrolment.
- Risk-Based Quality Management: oversight calibrated to the actual risk profile of the specific trial, documented prospectively.
MHRA inspectors will assess whether CtQ factors for the specific trial are traceable through the oversight architecture, whether monitoring decisions derive from those factors, and whether the rationale for each control is documented in a form that withstands scrutiny.
Delegation, Vendor Oversight, and Training
Sponsor accountability is non-delegable. Trial-related activities may be transferred to service providers. The transfer must be documented. Suitability must be assessed. Oversight must be active and evidenced, including work further subcontracted by the primary service provider.
Laboratory oversight is a defined sponsor responsibility under E6(R3). Monitoring plans must address important activities conducted away from the investigator site, including central image review and central laboratory operations.
Training must be proportionate to role and to the specific delegated activities on the specific trial. Documented evidence of training adequacy means should demonstrate competency for the functions performed, rather than relying solely on training completion record.
Computerised Systems
Systems used in trial conduct must be fit for purpose, validated proportionate to their function in that trial, and designed to protect data integrity across the trial life cycle. Validation must be documented and maintained. Audit trails must remain interpretable. Access controls, backup, disaster recovery, data transfer, and change control all require documented governance.
This applies to every system integral to participant safety or primary endpoint data: EDC, eTMF, eConsent, IRT, and central data platforms. Validation documentation that does not reflect the system’s actual function and risk in the specific trial will not satisfy the inspection standard.

Transparency: Statutory Duties from Today
For CTIMPs submitted on or after 28 April 2026, three transparency obligations are enforceable in law:
- Registration before first consent or within 90 days of approval, whichever is earlier.
- Results publication in the same registry within 12 months of the end of the trial.
- Accessible participant summary within 12 months of trial end, unless a deferral or waiver applies.
Failure to register or publish results is an offence under the Regulations. MHRA may take enforcement action, up to and including infringement notices and prosecution.
HRA has confirmed that registration on the EU Clinical Trials Information System alone does not satisfy the UK registration requirement. A separate qualifying UK registry entry is required.
Phase I CTIMPs involving only healthy volunteers, submitted from 28 April 2026, receive an automatic deferral of all three transparency obligations until 30 months after the end of the trial. The sponsor must still publish a minimal registration record on a publicly accessible registry within 90 calendar days of receiving combined approval from both MHRA and the REC, and before the first participant is recruited. Sponsors may choose not to use the deferral. A Phase I CTIMP that involves patients, even alongside healthy volunteers, does not qualify for automatic deferral.
Transparency: Statutory Duties from Today
For CTIMPs submitted on or after 28 April 2026, three transparency obligations are enforceable in law:
- Registration before first consent or within 90 days of approval, whichever is earlier.
- Results publication in the same registry within 12 months of the end of the trial.
- Accessible participant summary within 12 months of trial end, unless a deferral or waiver applies.
Failure to register or publish results is an offence under the Regulations. MHRA may take enforcement action, up to and including infringement notices and prosecution.
HRA has confirmed that registration on the EU Clinical Trials Information System alone does not satisfy the UK registration requirement. A separate qualifying UK registry entry is required.
Phase I CTIMPs involving only healthy volunteers, submitted from 28 April 2026, receive an automatic deferral of all three transparency obligations until 30 months after the end of the trial. The sponsor must still publish a minimal registration record on a publicly accessible registry within 90 calendar days of receiving combined approval from both MHRA and the REC, and before the first participant is recruited. Sponsors may choose not to use the deferral. A Phase I CTIMP that involves patients, even alongside healthy volunteers, does not qualify for automatic deferral.
Transitional Position
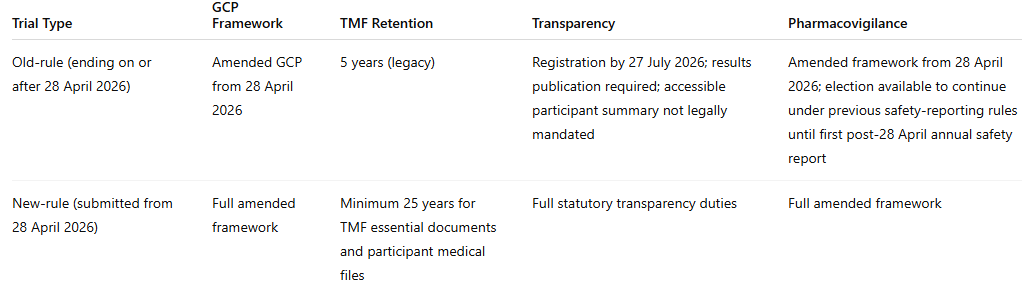
Sponsors with mixed portfolios need a documented transition assessment for each active trial with retention obligations confirmed, transparency deadlines assigned, and pharmacovigilance elections recorded.
Approval Timelines
Combined Review is now statutory. For new CTIMP applications submitted from today: initial review within 30 calendar days of valid application; up to 60 calendar days for the sponsor to respond to a Request for Further Information; final outcome within 10 calendar days of a complete response.
Substantial modifications are now handled through Route A or Route B.
Route A applies to modifications with a substantial impact on participant safety or rights, or on the reliability or robustness of data. A joint decision is expected within 35 calendar days of validation.
Route B applies to eligible lower-risk substantial modifications. On the MHRA side, automatic approval applies unless MHRA objects, requires Route A review, or confirms full assessment within the relevant period. Where REC review is required, ethics approval is not automatic and the sponsor must wait for the combined decision before implementation.
For new-rule trials, approval lapses after 2 years if no participant has been enrolled in the UK, unless an extension is granted. This lapse provision does not apply to old-rule applications.
Inspection Priorities
Under the amended framework, the focus will be on documented evidence across:
- CtQ factors defined before or alongside protocol development, with traceability through risk assessment, monitoring, data management, vendor oversight, and TMF evidence
- Monitoring and oversight decisions linked to trial-specific risk, not inherited from template practice
- Written agreements, suitability checks, oversight logs, escalation records, and subcontractor visibility for critical vendors
- Laboratory and central review oversight where these activities affect participant safety or important trial data
- Computerised systems governed through fit-for-purpose validation, access control, audit trails, backup, disaster recovery, and change control
- Transition assessments for active trials, including retention rules, transparency deadlines, and pharmacovigilance elections.
The practical message is clear. The amended UK framework rewards documented judgement, not procedural bulk. Sponsors need a quality system that shows what matters in each trial, why it matters, how it is controlled, and where the evidence sits.